Authored by Rhea Manohar MS2, Meghan Etsey MS3, Ariela Marshall MD on behalf of AMWA Gender Equity Task Force
Source: Chan, A. L., Guo, N., Popat, R., Robakis, T., Blumenfeld, Y. Y., Main, E., Scott, K. A., & Butwick, A. J. (2020, May 30). Racial and ethnic disparities in hospital-based care associated with Postpartum Depression. Journal of racial and ethnic health disparities. https://link.springer.com/article/10.1007/s40615-020-00774-y
Postpartum depression (PPD) is a critical health issue that affects approximately 10-20% of women in the United States (Gavin et al., 2005). PPD is characterized as a depressive disorder that begins post-birth and can last up to a year after pregnancy. For most, symptoms begin two to three days postpartum and can persist for weeks or longer. Symptoms of PPD range from those commonly attributed to depressive disorders, such as mood swings, loss of appetite, insomnia, fatigue, and increased irritability, to those more specific to pregnancy, including difficulty bonding with the baby and feelings of inadequacy related to parenting. In severe cases, PPD may lead to thoughts of harming oneself or the baby. Rarely, it may be associated with postpartum psychosis, which increases the severity of symptoms and the risk of life-threatening thoughts and behaviors (Healey et al., 2013).
If untreated, the effects of a mother’s PPD can have long-term detrimental effects on the behavioral, cognitive, and emotional developmental of the child (Halbreich, 2022). Infants of mothers experiencing PPD are at a higher risk of cognitive and emotional developmental issues due to weakened maternal-child attachment and reduced maternal responsiveness (Murray et al., 1996). One study found that disruptions in mother-infant bonding due to PPD can lead to decreased attentiveness, reduced emotional support, and long-term negative consequences for infant cognitive development (Bernard-Bonnin, 2004; Murray et al., 1996).
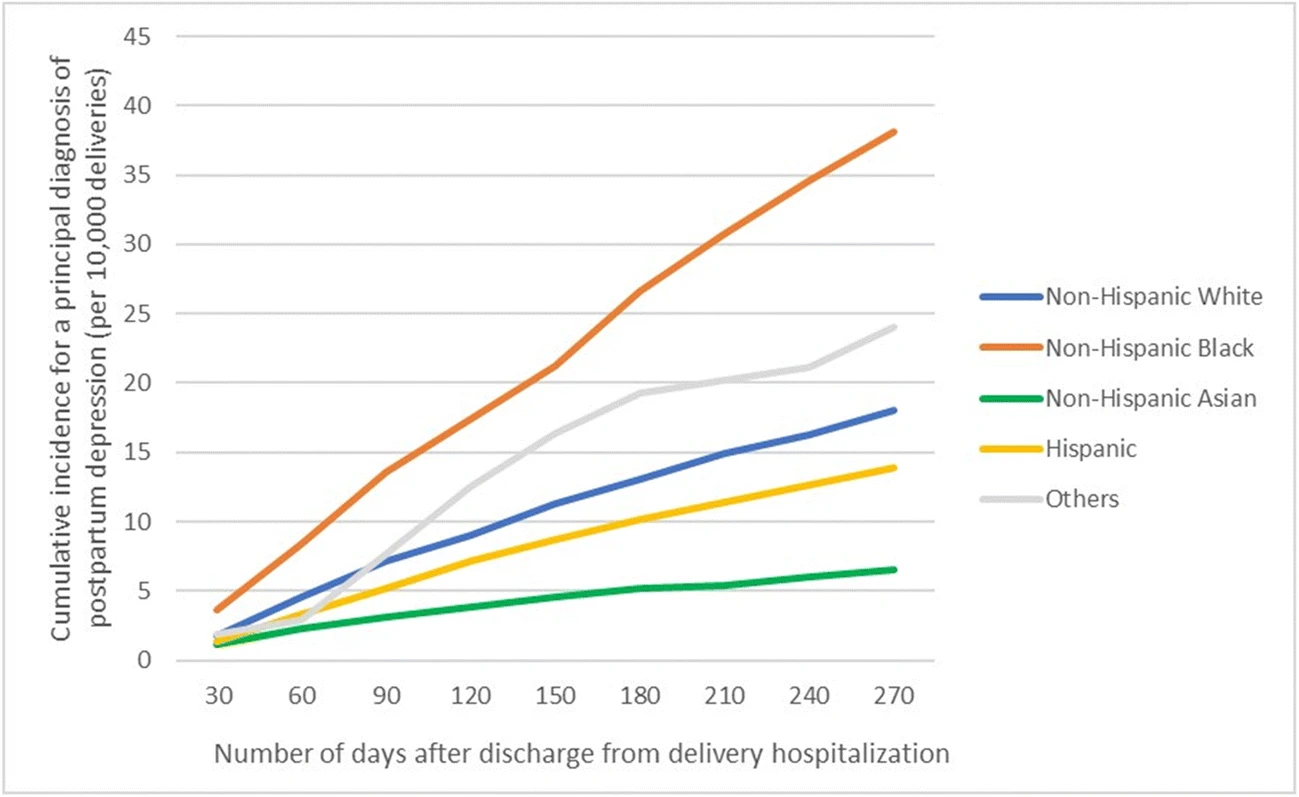
Despite affecting nearly one in eight women, PPD is frequently misdiagnosed or underdiagnosed (Gavin et al., 2005). While 19.2% of women experience a major depressive episode within the first three months postpartum , one survey found that 40% of women experiencing PPD symptoms fail to seek help. This decreased help-seeking behavior is attributed to feelings of shame, guilt, misunderstanding about treatment options, and stigma, which contribute to underdiagnosis (Gavin et al., 2005; Manso-Córdoba et al., 2020). Notably, the rate is significantly higher in women of color (Chan et al., 2020). Black/African American (B/AA) women, in particular, are affected by the significant racial and ethnic disparities in postpartum care incidence, screening, treatment, and resources (Chan et al., 2020; Kilgoe, 2021). PPD prevalence is disproportionately higher among B/AA women, who are three times more likely to experience PPD compared to their non-Hispanic White peers. This highlights the urgent need for more equitable maternal mental health support (Chan et al., 2020; Kilgoe, 2021).
Several factors contribute to the disproportionately higher prevalence of PPD among B/AA women, including:
- Cultural Stigma: Many B/AA women experience stigma surrounding mental health, leading to reluctance in seeking professional care or disclosing symptoms (Kozhimannil et al., 2011).
- Socioeconomic Stressors: Increased exposure to financial instability, employment challenges, and inadequate healthcare coverage contributes to the heightened risk of PPD in B/AA women (Kozhimannil et al., 2011).
- Discrimination and Bias in Healthcare: Implicit bias and a lack of culturally competent providers create additional barriers to diagnosis and treatment, leading to lower rates of screening and intervention for B/AA women (Hansotte et al., 2017).
- Lack of Social Support Systems: B/AA women often have limited access to community and familial support, which is a known protective factor against PPD (Pao et al., 2019).
Although screening tools like the Edinburgh Postnatal Depression Scale (EPDS) exist, their utilization remains inconsistent, particularly in marginalized communities (Sit & Wisner, 2009). One major concern is that these tools were developed primarily in clinical trials with non-Hispanic White women, raising questions about their effectiveness for B/AA women (Kozhimannil et al., 2011). Additionally, B/AA women are significantly less likely to receive follow-up care or treatment for PPD, including antidepressant prescriptions or therapy referrals (Kozhimannil et al., 2011; Hansotte et al., 2017). With limited systemic support, the responsibility too often falls on B/AA women to advocate for their own mental health in a system that has historically underserved them (Sandoiu, 2020).
To address these disparities, healthcare providers could integrate postpartum mental health education into prenatal care visits, ensuring that women and their families recognize potential symptoms of PPD before they occur (Kilgoe, 2021). Additionally,we advocate for provider training directed at how to better support B/AA women and others particularly at risk of PPD in maternal care settings (Hansotte et al., 2017). Approaching these conversations with cultural humility may alleviate some patient hesitance to care due to experiences with misdiagnosis and historical mistrust in healthcare providers within this community (Sandoiu 2020). Increasing research efforts that recruit racially diverse cohorts may also improve screening tool effectiveness and lead to better treatment outcomes for B/AA women (Kozhimannil et al., 2011). Lastly, we advocate for policymakers to allocate funding for PPD support services tailored to marginalized communities and develop programs that reduce barriers to care access (Summers et al., 2022).
A multifaceted approach is needed to address the disparity in PPD care. These approaches include early education, improved healthcare access, providers with cultural humility training, and targeted policy interventions. Expanding mental health education for both patients and providers can help reduce stigma and encourage early recognition of symptoms. Ensuring equitable healthcare access means not only increasing screening efforts but also removing barriers to follow-up care, such as cost, transportation, and provider availability. Additionally, training healthcare professionals in cultural awareness fosters more inclusive, patient-centered care that acknowledges and respects the unique challenges faced by B/AA women and other marginalized groups.
Beyond clinical efforts, policy changes are essential in bridging the disparity gap. This includes expanding insurance coverage for perinatal mental health services, increasing funding for community-based support programs, and investing in research that evaluates the effectiveness of screening tools across diverse populations. By implementing these strategies, the healthcare system can take meaningful steps toward closing the disparity gap and ensuring that all women—particularly those from historically underserved communities—receive the comprehensive care and support they need for their mental well-being.
References:
- Bernard-Bonnin, A.-C. (2004, October). Maternal depression and child development. Pediatrics & child health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724169/
- Chan, A. L., Guo, N., Popat, R., Robakis, T., Blumenfeld, Y. Y., Main, E., Scott, K. A., & Butwick, A. J. (2020, May 30). Racial and ethnic disparities in hospital-based care associated with Postpartum Depression. Journal of racial and ethnic health disparities. https://link.springer.com/article/10.1007/s40615-020-00774-y
- Manso-Córdoba, S., Pickering, S., Ortega, M. A., Asúnsolo, Á., & Romero, D. (2020). Factors Related to Seeking Help for Postpartum Depression: A Secondary Analysis of New York City PRAMS Data. International journal of environmental research and public health, 17(24), 9328. https://doi.org/10.3390/ijerph17249328
- Gavin, N. I., Gaynes, B. N., Lohr, K. N., Meltzer-Brody, S., Gartlehner, G., & Swinson, T. (2005, November). Perinatal depression: A systematic review of prevalence and incidence. Obstetrics and Gynecology. https://pubmed.ncbi.nlm.nih.gov/16260528/
- Halbreich, U. (2022, February 24). Long-term effect of persistent postpartum depression on children’s psychological problems in childhood. Journal of Affective Disorders. https://www.sciencedirect.com/science/article/pii/S0165032722002105
- Hansotte, E., Payne, S. I., & Babich, S. M. (2017, January 31). Positive postpartum depression screening practices and subsequent mental health treatment for low-income women in western countries: A systematic literature review – public health reviews. BioMed Central. https://publichealthreviews.biomedcentral.com/articles/10.1186/s40985-017-0050-y#:~:text=Physical%20barriers%20to%20PPD%20treatment,financial%20resources%2C%20and%20housing%20issues.
- Healey, C., Morriss, R., Henshaw, C., Wadoo, O., Sajjad, A., Scholefield, H., & Kinderman, P. (2013). Self-harm in postpartum depression and referrals to a perinatal mental health team: an audit study. Archives of women’s mental health, 16(3), 237–245. https://doi.org/10.1007/s00737-013-0335-1
- Kilgoe, A. (2021, July 26). Addressing the increased risk of postpartum depression for black women. NAMI. https://www.nami.org/Blogs/NAMI-Blog/July-2021/Addressing-the-Increased-Risk-of-Postpartum-Depression-for-Black-Women
- Kozhimannil, K. B., Trinacty, C. M., Busch, A. B., Huskamp, H. A., & Adams, A. S. (2011, June). Racial and ethnic disparities in postpartum depression care among low-income women. Psychiatric services (Washington, D.C.). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3733216/
- Murray, L., Fiori-Cowley, A., Hooper, R., & Cooper, P. (1996, October). The impact of postnatal depression and associated adversity on early mother-infant interactions and later infant outcome. Child development. https://pubmed.ncbi.nlm.nih.gov/9022253/
- Pao, C., Guintivano, J., Santos, H., & Meltzer-Brody, S. (2019, February). Postpartum depression and social support in a racially and ethnically diverse population of women. Archives of women’s mental health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6800248/
- Sandoiu, A. (2020, July 17). Postpartum depression in women of color: ‘more work needs to be done’. Medical News Today. Retrieved April 24, 2023, from https://www.medicalnewstoday.com/articles/postpartum-depression-in-women-of-color-more-work-needs-to-be-done#2
- Sit, D. K. Y., & Wisner, K. L. (2009, September). Identification of postpartum depression. Clinical obstetrics and gynecology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2736559/#:~:text=Edinburgh%20Postnatal%20Depression%20Scale%20(EPDS,to%20childbearing%20is%20the%20EPDS.
- Summers, J., Levitt, M., & Handel, S. (2022, August 16). Postpartum care falls short for black women. One mother is trying to fix that. NPR. https://www.npr.org/2022/08/16/1117762246/postpartum-care-falls-short-for-black-women-one-mother-is-trying-to-fix-that
About the Authors
 Rhea Manohar, MS2
Rhea Manohar, MS2
Rhea Manohar is a second year medical student from St. George’s University. She has a Masters in Public Health with a concentration in Maternal and Child Health from George Washington University Milken Institute of Public Health and a Bachelors of Science in Microbiology, Immunology, and Public Health from the University of Miami. She served as Co-VP of OB/GYN Education for St. George’s University’s Women in Medicine chapter in St. George, Grenada where she developed and implemented hands-on workshops to further reproductive health issues and bolstered medical students abilities to navigate physician-patient communication. Prior to medical school, she was a Research Associate for Fors Marsh Group, where she led qualitative and quantitative public health research and campaign development for federal agencies (e.g., CDC, NIH, DHHS, CPSC). She is also a member of the Gender Equity Task Force and Reproductive Health Coalition within the American Medical Women’s Association. When she is not pursuing medicine, you can find her reading, exploring artistic passions, and spending time connecting with friends and family.
 Meghan Etsey, MS3
Meghan Etsey, MS3
Meghan is a third year medical student from St. George’s University. She has a Bachelors of Arts in Biology and a Bachelors of Arts in Nutrition and Dietetics from Bluffton University in Bluffton, Ohio. She served as the President of the St. George’s University’s Women in Medicine chapter in St. George, Grenada where she expanded relationships with the community and worked towards educating women and helping the youth. She is also a member of the Gender Equity Task Force and Sex and Gender Health Collaborative Committees within the American Medical Women’s Association. When she is not pursuing medicine, you can find her with her friends and family on different road trips and adventures exploring the world.
 Ariela Marshall, MD
Ariela Marshall, MD
Dr. Ariela Marshall is a Harvard-trained physician and an internationally renowned advocate, career development advisor, and mentor. Dr. Marshall specializes in bleeding and clotting disorders, especially as they relate to women’s health. She has worked at Mayo Clinic and the University of Pennsylvania and currently practices part-time as a consultative hematologist at the University of Minnesota. In addition to her clinical work, Dr. Marshall is a highly respected leader, mentor, and speaker. She is an active leader with the American Society of Hematology (where she led efforts to found the Women in Hematology Working Group and currently holds seats on the Women in Heme Working Group, Committee on Communications and Media Experts Subcommittee) and American Medical Women’s Association (leading the Infertility Working Group and holding seats on the Gender Equity Task Force). She is the Chief Innovation Officer at Women in Medicine and the Curriculum Chair at IGNITEMed, which are both 501(c)(3) nonprofit organizations dedicated to promoting career development for women in medicine. She speaks regularly on a national and international scope to discuss her efforts to advance career development and mentorship for physicians, gender equity, fertility/infertility awareness, parental health and wellbeing, reproductive health and rights, and work-life integration.