Authors: Meghan Etsey MS3, Rhea Manohar MS2 MPH, Rosy Thachil MD on behalf of the Gender Equity Task Force
Source: Vasisht, K. P., Nugent, B. M., & Woodcock, J. (2021, May 14). Progress and opportunities for women in clinical trials: A look at recent data and initiatives from the U.S. FDA. Science Direct. https://www.sciencedirect.com/science/article/pii/S2666634021001598
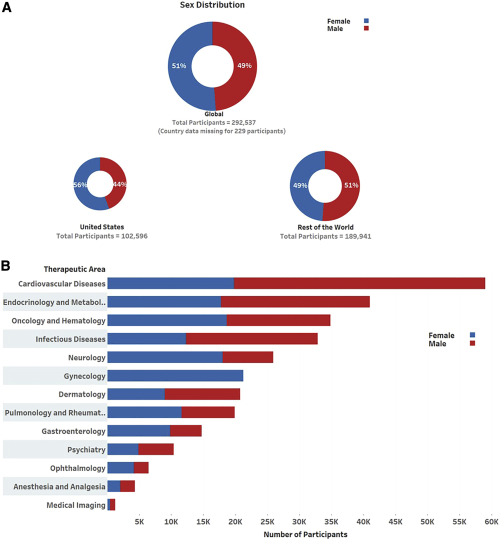
In recent years, there has been increasing awareness of gender inequity in various areas, including healthcare. One critical area that historically gone unnoticed is the representation of women in clinical trials. This blog explores the implications of gender inequity in clinical trials and calls for more inclusive research practices. Despite the fact that women comprise approximately half of all clinical trial participants, they are often underrepresented in critical studies, compared to their estimated disease burden (e.g., heart disease, autoimmune disorders, oncology, neurology). A 2020 study found that only 38% of participants in cardiovascular trials were women (Jin et al., 2020). While women comprised 46.9% of participants in an analysis of 160 oncology clinical trials, it was found that women were underrepresented in kidney and invasive oncology trials (Perera et al., 2023). In comparing nephrology and genitourinary studies in 2000 and 2020, despite incurring 45.2% of disease burden, women made up only 41.7% of participants (Steinberg et al., 2021). These studies highlight a key gap in research participation and consequently analysis and evaluation of efficacy for treatment protocols and interventions for women.
The impact of gender inequity in clinical trials can be profound. When women are underrepresented, the efficacy and safety of treatments may be poorly understood, leading to suboptimal healthcare outcomes for potentially half the general population (Bairey Merz et al., 2017; Vasisht et al., 2021). This inequity can exacerbate existing health disparities, particularly in populations already facing barriers to healthcare access (National 2022). Recruitment and inclusion in clinical trials for individuals from rural settings as well as those from racial and ethnic minorities remains a critical concern across disciplines. The scientific limitation of the generalizability of the trial results for these subsets of women are compounding the health inequities that pervade in medical and research accessibility (Bierer et al., 2022).
Several barriers contribute to the underrepresentation of women in clinical trials, including:
- Historical Precedents: The legacy of excluding women from research due to concerns about potential risks related to pregnancy (Petrie-Flom 2021).
- Socioeconomic Factors: Women may face logistical challenges, such as childcare responsibilities or economic constraints, that prevent them from participating (Gaur et al., 2024).
- Recruitment challenges: Additional screening protocols are often implemented for women of child-bearing age including serum or urine β-hCG samples and contraception checks (Persampieri 2021).
- Data Integrity: Concerns over increased variability in the data impacting intervention outcomes due to the fluctuation of hormones in younger women continue to impede recruitment (Mager & Liu, 2016).
To address these issues, it is essential to implement inclusive guidelines. Regulatory bodies should enforce stricter guidelines for gender representation in clinical trials (Adams et al., 2022). Some progress has been made with the implementation of the NIH Revitalization Act of 1993, which mandated NIH funded clinical trials to include women, and more recently the 2024 White House Initiative on Advancing Women’s Health Research and Innovation. Despite the additional focus and added incentives for including women in clinical trials, gaps still remain (Colino 2024).
Additionally, it is critical to raise awareness among healthcare providers and the public about the importance of gender equity in research (Adams et al., 2022). While women are categorically underrepresented in research across the board, a newfound focus on obstetrics and gynecology research and clinical trials could encourage enrollment. Increasing visibility and encouraging clinical trials in areas, such as menopause, endometriosis, and obstetrical complications can help fill a critical knowledge gap (Colino 2024). Community engagement can help shine a light on the importance of clinical trial participation and build trust for future recruitment efforts (Bierer et al., 2022).
Lastly, researchers can encourage women participation by addressing the socioeconomic and interventional factors that lead to decreased recruitment. Incorporating necessary adaptations to study protocols to account for biological and physiological differences can not only encourage participation but also improve generalizability of the trial efficacy (Goldstein et al., 2024). As women are more likely to face logistical barriers to participation, offering additional services or incentives, such as childcare and transportation, can alleviate this burden. In other cases, utilizing technology and remote participation options can help mitigate logistical barriers for women, especially those of color and in rural settings (Adams et al., 2022; Bierer et al., 2022). Altogether, gender inequity in clinical trials is a pressing issue that requires immediate attention. By advocating for more inclusive practices, we can ensure that all populations receive the benefits of research advancements.
References
- Adams, D. V., Long, S., & Fleury, M. E. (2022). Association of remote technology use and other decentralization tools with patient likelihood to enroll in cancer clinical trials. JAMA Network Open, 5(7), e2220053. https://doi.org/10.1001/jamanetworkopen.2022.20053
- Bairey Merz, C. N., et al. (2017). Cardiovascular disease in women: A statement for healthcare professionals from the American Heart Association. Circulation, 135(12), e1000-e1020. 10.1161/01.cir.96.7.2468
- Bierer, B. E., Meloney, L. G., Ahmed, H. R., & White, S. A. (2022). Advancing the inclusion of underrepresented women in clinical research. Cell reports. Medicine, 3(4), 100553. https://doi.org/10.1016/j.xcrm.2022.100553
- Colino, S. (2024, November 1). Does the gender gap in medical research still exist?. Time. https://time.com/7171341/gender-gap-medical-research/
- Gaur, P., Ganguly, A. P., Kuo, M., Martin, R., Alvarez, K. S., Bhavan, K. P., & Kho, K. A. (2024). Childcare needs as a barrier to healthcare among women in a safety-net health system. BMC Public Health. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-024-19125-1
- Goldstein, K. M., Kung, L. C. Y., Dailey, S. A., Kroll-Desrosiers, A., Burke, C., Shepherd-Banigan, M., Lumsden, R., Sims, C., Schexnayder, J., Patel, D., Cantrell, S., Sheahan, K. L., & Gierisch, J. M. (2024, January 2). Strategies for enhancing the representation of women in clinical trials: An evidence map – systematic reviews. BioMed Central. https://doi.org/10.1186/s13643-023-02408-w
- Jin, X., Chandramouli, C., Allocco, B., Gong, E., Lam, C. S. P., & Yan, L. L. (2020). Women’s participation in cardiovascular clinical trials from 2010 to 2017. Circulation, 141(7), 604–605. https://doi.org/10.1161/CIRCULATIONAHA.119.043594
- Mager, N. A. D., & Liu, K. A. (2016, March 12). Pharmacy practice. Pharmacy Practice. https://www.pharmacypractice.org/index.php/pp/article/view/708
- National Academies of Sciences, Engineering, and Medicine. (2022). Improving the representation of women and underrepresented minorities in clinical trials and research. The National Academies Press. https://www.nationalacademies.org/our-work/improving-the-representation-of-women-and-underrepresented-minorities-in-clinical-trials-and-research
- Perera, N. D., Bellomo, T. R., Schmidt, W. M., Litt, H. K., Shyu, M., Stavins, M. K. A., Wang, M. M., Bell, A., Saleki, M., Wolf, K. I., Ionescu, R., Tao, J. J., Ji, S., O’keefe, R. M., Pun, M., Takasugi, J. M., Steinberg, J. R., Go, R. S., Turner, B. E., & Mahipal, A. (2023). Analysis of Female Participant Representation in Registered Oncology Clinical Trials in the United States from 2008 to 2020. Oncologist, 28(6), 510-519. https://doi.org/10.1093/oncolo/oyad009
- Persampieri, L. (2019). Gender and Informed Consent in Clinical Research: Beyond Ethical Challenges. BioLaw Journal – Rivista Di BioDiritto, (1S), 65–87. https://doi.org/10.15168/2284-4503-401
- Petrie-Flom Center. (2021, April 16). Pregnant in clinical trials: Balancing safety and autonomy. Harvard Law School. https://petrieflom.law.harvard.edu/2021/04/16/pregnant-clinical-trials-safety-autonomy/
- Steinberg JR, Turner BE, Weeks BT, et al. Analysis of Female Enrollment and Participant Sex by Burden of Disease in US Clinical Trials Between 2000 and 2020. JAMA Netw Open. 2021;4(6):e2113749. https://doi.org/10.1001/jamanetworkopen.2021.13749
- Vasisht, K. P., Nugent, B. M., & Woodcock, J. (2021, May 14). Progress and opportunities for women in clinical trials: A look at recent data and initiatives from the U.S. FDA. Science Direct. https://www.sciencedirect.com/science/article/pii/S2666634021001598
About the Authors
 Meghan Etsey, MS3
Meghan Etsey, MS3
Meghan is a third year medical student from St. George’s University. She has a Bachelors of Arts in Biology and a Bachelors of Arts in Nutrition and Dietetics from Bluffton University in Bluffton, Ohio. She served as the President of the St. George’s University’s Women in Medicine chapter in St. George, Grenada where she expanded relationships with the community and worked towards educating women and helping the youth. She is also a member of the Gender Equity Task Force and Sex and Gender Health Collaborative Committees within the American Medical Women’s Association. When she is not pursuing medicine, you can find her with her friends and family on different road trips and adventures exploring the world.
 Rhea Manohar, MS2
Rhea Manohar, MS2
Rhea Manohar is a second year medical student from St. George’s University. She has a Masters in Public Health with a concentration in Maternal and Child Health from George Washington University Milken Institute of Public Health and a Bachelors of Science in Microbiology, Immunology, and Public Health from the University of Miami. She served as Co-VP of OB/GYN Education for St. George’s University’s Women in Medicine chapter in St. George, Grenada where she developed and implemented hands-on workshops to further reproductive health issues and bolstered medical students abilities to navigate physician-patient communication. Prior to medical school, she was a Research Associate for Fors Marsh Group, where she led qualitative and quantitative public health research and campaign development for federal agencies (e.g., CDC, NIH, DHHS, CPSC). She is also a member of the Gender Equity Task Force and Reproductive Health Coalition within the American Medical Women’s Association. When she is not pursuing medicine, you can find her reading, exploring artistic passions, and spending time connecting with friends and family.
 Rosy Thachil, MD, FACC, co-chair of AMWA’s Gender Equity Task Force, is a quadruple board-certified cardiologist, serving as Director of the Cardiac Intensive Care Unit at Elmhurst Hospital Center, and Assistant Professor at Mount Sinai College of Medicine in New York. Dr. Thachil’s clinical interests include critical care cardiology/acute cardiovascular care and health disparities. In addition to addressing cardiovascular disease, she is passionate about advancing womens’ roles in medicine/leadership. She also serves on American College of Cardiology Critical Care Leadership Council and she is a candidate at Wharton’s executive MBA program (‘25), and holds certificates in physician leadership and bioethics.
Rosy Thachil, MD, FACC, co-chair of AMWA’s Gender Equity Task Force, is a quadruple board-certified cardiologist, serving as Director of the Cardiac Intensive Care Unit at Elmhurst Hospital Center, and Assistant Professor at Mount Sinai College of Medicine in New York. Dr. Thachil’s clinical interests include critical care cardiology/acute cardiovascular care and health disparities. In addition to addressing cardiovascular disease, she is passionate about advancing womens’ roles in medicine/leadership. She also serves on American College of Cardiology Critical Care Leadership Council and she is a candidate at Wharton’s executive MBA program (‘25), and holds certificates in physician leadership and bioethics.